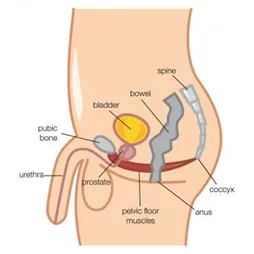
Pelvic floor muscle injury in labour
3 August 2016 Pregnancy, Women's Health
Recovering after 3rd and 4th Degree Tears Unfortunately, during birth, women can experience perineal tearing. The perineum is the area between the vaginal opening and the back passage. A woman can suffer from varying degrees of tearing, with some short term, but also long term effects on pelvic floo...
Read More