Pregnancy and Incontinence
World Continence Week raises awareness for pregnant women world-wide
Urinary incontinence is a loss of bladder control which results in leaks of urine. This can be stress incontinence which is leaking urine with a cough, sneeze, laugh, exercise (including running, jumping, lifting weights), or even during sex. Or it can be urge incontinence which is a strong overwhelming desire to urinate and losing control before reaching the bathroom. Women over the age of 35 and women with a high BMI have a greater risk of both stress and urge incontinence during pregnancy and after birth.
Why can women suffer from incontinence during pregnancy?
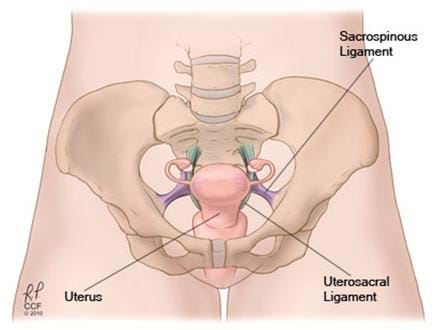
It is quite common for women to develop some form of incontinence during pregnancy, and the most common form is stress incontinence. There are many reasons for this but the biggest reason is the extra weight of the unborn baby and the pressure of the uterus on the bladder. This is why pregnant women can often only develop incontinence in their third trimester. Sometimes constipation can also lead to incontinence because of the added pressure of the full bowel on the bladder.
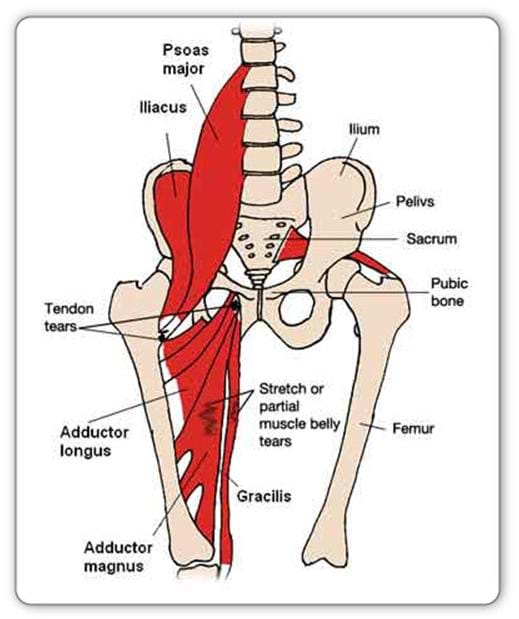
One other major reason is the large hormonal changes in pregnancy, which make the connective tissue including the ligaments very soft and lax. Women need their joints and tissues to be more elastic (particularly around the pelvis) for childbirth, but this also reduces the support of the bladder, hence why some women will leak. This extra weight and pressure combined with the laxity of the joints puts added pressure on the pelvic floor muscles. Pelvic floor muscles will then fatigue quicker, and if the pelvic floor muscles are already weak, it can lead to incontinence.

Why is incontinence prevalent after pregnancy and birth?
Leaking is common in one in three women after childbirth. Sometimes women lose their ‘connection’ (brain message to muscle) to their pelvic floor muscles after childbirth and the muscles weaken. Perhaps it is the pain associated with the birth and its interventions which cause this. This weakness means the muscles can’t tighten around the urethra efficiently and a leak can occur. Sometimes these pelvic floor muscles can become weaker due to prolapse, or sagging, of any of the pelvic organs, which puts extra load and pressure on the pelvic floor muscles.
After childbirth, the biggest risk factor for stress incontinence is having a vaginal delivery, especially if instruments such as forceps or vacuum were used, as these can injure pelvic nerves and muscles. Other risk factors include having your first baby, having a large baby over 4 kilograms, having a long labour, especially the second stage of labour, and having a difficult vaginal delivery, which involve stitches or tears around or outside the vagina. If a woman has tearing of her perineum or prolapse of her bowels, she may also develop faecal incontinence. Women who have had caesarian sections can also develop incontinence especially if their pelvic floor muscles are weakened from the pressure of the uterus.
Is there anything that can be done to prevent pregnancy-related incontinence?
It is important for all women to do their pelvic floor exercises during pregnancy and after childbirth. An excellent way to do these exercises and help to manage or prevent incontinence is to join a Pregnancy Pilates group exercise program, such as those offered at The Fix Program. After you’ve given birth, it is highly advised to see a women’s health physiotherapist if you are experiencing any incontinence to make sure you get the therapy you need. At The Fix Program our women’s health physiotherapists are highly skilled in assessing pelvic floor function and can help you manage any incontinence as well as treat any prolapse or scar tissue you might have post-birth.